Teal is the awareness color of ovarian cancer. Women of Teal is a play on the words "Man of Steel" used to describe Superman. I have found my fellow ovarian cancer survivors to be the strongest, most helpful women in the world. They are truly Women of Teal!
December 30th marks my 8th year writing this blog.When I first began I knew I wanted to raise awareness of the disease, share my story with other women diagnosed with ovarian cancer and disseminate information about cancer survivorship. I wasn't sure how long I would continue posting to Women of Teal. Would I be well enough to post? Would I run out of things to write about?
This is my eighty-first post of the year, more than last year but not as high as 2009 or 2012 years in which I wrote well over one hundred and fifty posts. When looking back over the past year's posts the majority of what I wrote related to ovarian cancer research ( SGO and ASCO annual meetings ) as
well as study results reported in journal articles.
During the month of September I took the GCAM ( Gyn Cancer Awareness Month) Challenge. I posted each day on gyn cancer topics from ovarian cancer - risks, treatment, genetics to cervical cancer, HPV and precision medicine. In other posts this year I've written about:
books I've read and the book I wrote with Dr Don Dizon
what I learned about the CA-125 test and the two lab processes to measure it
NED the Band and the Movie
The Astra Zeneca Bloggers Conference
Presentations I made to Rutgers University AMSA students and Eye for Pharma's Patient Summit
There were times though when I wrote about more personal issues. I miss many of my teal sisters and wrote frequently about the effect they had on my life. I look forward to continuing to write in 2016. I do this with the hopes that sharing what I learn at conferences or reporting on the latest research will be beneficial to my followers.
Thank you to all who followed, commented or e-mailed me this year I appreciate interacting with all of you. Please let me know if there are any topics you would like me to write about in 2016 .
Last June, when I attended the ASCO annual meeting I was fascinated by a presentation by Dr Usha Menon on the UK Collaborative Trial of Ovarian Cancer Study (UKCTOCS) using the ROCA (Risk of Ovarian Cancer Algorithm) test. I wrote about it here.
Earlier this month I was contacted by a representative of the PR firm that is representing Abcodia, a company that develops early detection tests for cancer. On December 2, 2015 Abcodia launched the ROCA (Risk of Ovarian Cancer Algorithm) test here in the US. After finding and reading my blog, the firm contacted me to share that the test was now available. Of course I was interested in learning more about this test that was now available in 5 states - Texas, Massachusetts, Illinois, Arizona and my home state of New Jersey. You can find the press release at http://www.abcodia.com/news_021215.php.
We conversed via e-mail and then I had a teleconference with the PR firm's representative as well as the representatives from Abcodia. Abcodia's responses to my questions are shown below in quotes and italics. I have permission from Abcodia to share the information provided.
What is the difference between the ROCA test and the CA-125, which is one component of the ROCA test? "The ROCA Test does not use CA-125 with a fixed cutoff, instead, ROCA establishes a patient’s baseline, and then evaluates her CA-125 pattern over time." (CA-125 uses a fixed cut-off of either 35 u/ml or 20 u/ml depending on which test protocol is followed. "ROCA incorporates the CA-125 result (and all the following CA-125), and, factors in age, menopausal status and high risk factors, which affect CA-125 levels. ROCA takes all of this data on one patient and creates a unique profile for her. ROCA then compares her profile to known profiles in a database of thousands of women to see if her profile more closely resembles that of women who have cancer or women who do not have cancer. The ROCA Test reports a numerical score which represents a woman’s risk of having ovarian cancer (e.g. 1 in 5,000) now. The risk score is categorized as Normal, Intermediate or Elevated as a guide for clinical decisions by your doctor."
Who is the ROCA test meant for and when should they have it? The ROCA test is meant for women in the general population who are "Between 50 and 85 years and have been through menopause; or" high risk women "Between 35 and 85 years with a family history of ovarian and/or breast cancer, are of Ashkenazi Jewish descent with a known family history of ovarian or breast cancer, or have tested positively for BRCA1, BRCA2 or Lynch syndrome gene mutations." The CA-125 may be used for high risk women only. The test would be similar to "Routine testing, just like you would a physical or mammogram." Currently the CA-125 with a fixed cutoff is sometimes used for high risk women only when advised by their physicians. As many of my readers know, the CA-125 is used by gynecologic oncologists to manage the care of women who have been diagnosed with ovarian cancer.
How does the ROCA test compare to the CA-125 in terms of how well it detects ovarian cancer?"When combined with appropriate clinical follow-up, the ROCA Test has been shown to detect more than twice as many ovarian cancers before the current CA-125 35U/ml fixed cutoff. As a screening tool by itself, CA-125 is not reliable and has not been shown to improve outcomes for women with ovarian cancer."
How does a woman go about getting the test? She fills out a form online to see if she is eligible and orders the kit. Then she finds a referring physician (OB-GYN or primary care physician) to sign the request for the test and the blood work. "Abcodia is proactively educating OBGYNs, has a dedicated phone line and online materials specifically for healthcare professionals."
What is the cost of the test and is it covered by Medicare, other insurances? "The cost of each ROCA Test is $295. This includes the cost for the Iggbo blood draw service, who will have a trained phlebotomist come to a doctor’s office, a patient’s home or other location of the patient’s choice to draw blood. Iggbo will then ship the blood sample via FedEx to Abcodia’s laboratory." Abcodia's lab is a CLIA, registered lab. Currently the test is not covered by Medicare or other insurances. "Abcodia does plan to seek regulatory and reimbursement approvals"
Can a woman get the CA-125 drawn at a different lab and then submit it to Abcodia? It is recommeded that the blood draw be through Abcodia's blood draw partner, Iggbo. A patient can have her blood drawn at her physician's office or a hospital if a phlebotomist is available. All samples do need to be tested at the Abcodia lab to insure there is no lab to lab variability. CA-125 test results from other labs (Quest, Labcorp) for use with the test are not accepted.
What happens after the initial result? "The frequency of the ROCA test will be determined by the woman's doctor based on her risk factors for ovarian cancer and the ROCA test result. Post menopausal women with no additional risk factors will likely have one test per year. Women at high risk for ovarian cancer , will complete the test more frequently, at a minimum three times per year and may include a Transvaginal Ultrasound (TVU). If the result falls outside of the normal range(intermediate or elevated) a doctor may recommend a repeat ROCA test within the next six weeks to three months.Patients may also be referred for a transvaginal ultrasound scan of the ovaries or other possible clinical assessments. "
Does the women pay $295 each time she has a follow-up test?"After a patient takes her first test, Abcodia offers the patient several options: 1. The patient can pay per test ($295) for each test. 2. The ROCA Test Subscription: one for high risk patients and one for the general population. Abcodia will offer patients a 2 year subscription that includes the Iggbo blood draw, repeat ROCA tests and TVU (Transvagina Ultrasound) as a result of intermediate, elevated or severe ROCA result. 3. Interest free payment plans."
Why is the test available in only five states ?Starting in five states will allow the test process to be optimized. The delay with other states is due to each individual state's permit application period and process. Some are longer than others.
This video is an overview of how the ROCA test works.
I have charted my CA-125 results since my initial diagnosis. So monitoring the trends in CA-125 makes sense to me. But there is one caveat, there is a small percentage of women, like myself, who have a CA-125 result that is normal and disease may be still present. My CA-125 was normal at 17 u/ml, when I learned via CT scan that I had recurred on my liver and spleen. So woman whose CA-125 does not rise may not benefit from this type of screening.
I still had a few questions about applying this test to the general public. I wondered if the ROCA test would find the disease at an earlier stage and if the survival would be longer for women whose disease was detected by this test. I did not have to wait too long for some of the answers because on December 17th the results were published in the Lancet journal.
Details: ClinicalTrials.gov, number NCT00058032 Randomized Trial: 202,638 Post menopausal women 50-74 from England, Wales, Northern Ireland Three arms: 1. Annual Multimodal Screening (MMS) using CA-125 and risk algorithm ( 50,624 women ). I call this arm the ROCA test but will use MMS when discussing the study. 2. Annual transvaginal ultrasound (TVU) (50,623 women) 3. No screening ( 101,299 women) . The distribution ratio was 1:1:2.
OC was diagnosed in 1282 women of all women 630 cases in the unscreened women with 347 deaths 338 cases in the screened with CA-125 and ROCA 148 deaths 314 cases in the ultrasound screen group and 154 death.
One analysis showed less deaths in the MMS and TVU groups but the difference was not significant. Mortality reduction using the Cox Model for years 0-14 showed a 15% reduction in deaths in the MMS group versus the control group. And there was an 11% reduction in mortality in the TVU group versus the control group. Graphs of the control versus MMS and control vs TVU are the same up to about 10 years. If you look at specific time periods there is a change in mortality reduction. For MMS the 0-7 time period showed an 8% reduction vs control and for 7-14 year time period there was a 23% reduction in mortality versus the control.
A second analysis which removed women,who had ovarian cancer before the screening of the trial began and who died early on in the study ( "prevalent cases" in which the change point in the CA-125 occurred before enrollment in the study) found that the MMS group had an average of 20% less deaths for the entire study ( 0-14 years) .
You may view watch this video ( 2hours 40 minutes) of the UKCTOCS Ovarian Cancer Mortality Results Meeting ( includes psychosocial evaluations of participants as well as mortality data ):
During this video it was stated that these early results from the UKCTOCS ( no significant p value) is similar to the results of the late effect seen in the PSA European study( for prostate cancer) and time is needed to follow-up and confirm late effects.
Discussion of the results: There were media articles ( NYT) written stating that early detection of ovarian cancer was now possible because of this test. Medpage- Ovarian Cancer Screening Study Falls Short
OCNA - “These
initial results are promising for the ovarian cancer community, but
there is much more data analysis needed in the coming months to
determine the true impact on the future of early detection testing for
ovarian cancer. We are looking forward to discussions with the community
in the coming months to understand how ROCA may fit into the prevention
of ovarian cancer."
For me questions still remain. What was the grade of the women that died during the study? I know from the previous JCO article that 82% of the women in the study diagnosed with Ovarian Cancer were high grade. How did that correlate with those who died.
From the JCO article 41 % of the women dx with OC in the MMS arm were stage 1 or 2. How does that relate to their mortality?
What I wish I knew: Does the ROCA / CA-125 test work on women earlier than age 50? Those that are pre-menopausal?
If you were able to look at the BRCA status of the women in the study would that effect the results? (Is the test better on those with a BRCA mutation?
As many others during the past few days have said. This is promising but more work needs to be done.
I upgraded my phone the other day. In case the data transfer did not work correctly, I decided to go through my contacts and make sure I had all the important phone numbers.
Right up front under letter B was Jeanne Burton. We met each other at the Rutgers Cancer Institute of NJ support group . We talked a few times by phone but once she moved back to Maine it was mostly texts and e-mails. She would text me updates- "Found a palliative care doctor", "really like my new oncologist" and " you should come visit" . I wrote about her move to Maine here. I regret never getting up to Maine before she passed on June 21, 2015. I wrote about the choices she made here. I deleted her contact info.
Then under C was Courtney Clifford. Courtney and I became friends in 2006 at the LiveSTRONG Survivors Summit. She experienced the same symptoms I did and was diagnosed a few months after I was. The difference was she was 23 years old and I was 50. She was the youngest woman I had ever met who had ovarian cancer. We kept in touch through the years and saw each other at the 2008 LiveSTRONG Summit in Ohio her home state. I appreciated her long distance friendship. Sadly I had to write about her passing in 2012 (http://womenofteal.blogspot.com/2011/02/courtney-1982-2011.html) . I deleted her cell phone number.
I got to the letter F and there she was - Pam Favocci. I met Pam at the Rutgers Cancer Institute of NJ Support Group. Over the years we became close friends and together we took part in many awareness activities together. On December 14th she will be gone 3 years. I honored her in A Friendship Ended Too Soon. I deleted her home number.
Then I got to J and there was Linda Juarez. A few years ago my gyn onc asked if I would talk to Linda. Out of that simple introduction a friendship grew. We both recurred in 2008 and that brought us even closer. We had late night phone calls about clinical trials and texts would arrive during her frequent hospital visits. She passed in May this year and I wrote about her here. I deleted her number.
I was a bit surprised when I got to T and I found Rita Kay Thomas' phone number. I forgot I had her phone number in my phone. When I was in college I first met Rita Kay - she was the Assistant Athletic Director. Who knew that our paths would cross 30+ years later. Ovarian Cancer took this amazing woman too soon in October 2012. I wrote about our friendship here. I deleted her number.
I thought about each of those women as I deleted their numbers.
I hated doing it because such a simple action triggered a deep sadness.
The tweet links to a blog post which describes how a system built by Watson Health using Merge Healthcare data and machine learning can provide an initial recommendation. The recommendation will be based on accessing patient symptoms and cross referencing images with previously diagnosed scans. Basically radiologists could be replaced by machines. The blog ends with recommendations for radiologists to "step into the light".
In the past 10 years, my care has included 21 CT scans, 2 PET/CTs, and 11 mammograms. In that time period I have only met one radiologist. Back in 2005 after being diagnosed with ovarian cancer my gyn-onc sent me for a mammogram to insure that I did not have breast cancer. I had a script to go that day for a mammogram so they squeezed me into the schedule. After finishing, the technician asked me to wait for a minute in the room. In walked the radiologist who had called my gyn-onc with the results. They did not want me to wait over the weekend for the results so the radiologist told me my mammogram images were clear. I thanked him and he wished me luck with the chemotherapy treatments.
In every other instance the radiologist who read my scans was behind the scenes. I have copies of the slides of each scan on CDs and also the written report for each scan. The report includes the name of the radiologist who read the scan and wrote the report. The group I use for my scans has over 50 radiologists listed on their web page. After years of scans I began to noticed that some of my scans were read by the same person and that was comforting.
In October 2008, it was a CT scan that found my recurrence on
my liver and spleen. (My CA-125 was normal).
So I have lots of reasons
to thank the wonderful radiologists at University Radiology for the behind the scenes care they provide.
I am grateful for
my husband
my children and their spouses
my grandsons
my family - sister, brother-in-laws, sister-in-laws, nieces, nephews, cousins,
my dog and my grandpups and grandkittens
my friends near and far
followers of this blog
There are many organizations that raise funds for cancer research. A simple Google search of "organizations that support ovarian cancer research " will give you over 900,000 results. Some of these are large national non-profit organizations with offices and multiple employees with large budgets that support research in addition to other programs such as awareness and legislative advocacy.
But there are also many small, local non-profit organizations throughout the US whose efforts should not go unheralded. They have all volunteer boards, meet in public spaces or around someones dining room table and still manage to make a difference and change the research landscape by supporting established research programs for early detection and treatments as well as young researchers.
Yesterday, I was invited by the GRACEful Hope Foundation to attend their presentation of a check for $30,000 to support ovarian cancer research at Memorial Sloan Kettering Cancer Center. For over 4 years now the GRACEful Hope Foundation lead by the Rocha Family and friends have supported ovarian cancer research to honor the memory of Grace and Erika Rocha.
Another NJ non-profit, Kaleidoscope of Hope Foundation , earlier this year presented grant awards to RACHEL N. GRISHAM, M.D.,Memorial Sloan Kettering Cancer Center, to support her research on Deciphering the Biologic Predictors of Response to Targeted Therapy in Low Grade Serous Ovarian Cancer ,LILIE LIN, M.D. , University of Pennsylvania, to support her Pilot Study of a Novel PARP Inhibitor PET Tracer in Ovarian Carcinoma and continued funding the project of GEORGE PRETI, Ph.D., Monell Chemical Senses Center, A Novel
Multidisciplinary Approach to Development of an Effective Ovarian Cancer
Screening Diagnostic using Volatile Biomarkers. KOH has provided over 2.7 million dollars to support ovarian cancer research in the past 15 years.
Since 2010, The Teal Tea Foundation has supported Dr. Eric A. Ariazi, Fox Chase Cancer Center, Dr. Elyce Cardonick, Cooper Cancer Institute, Dr. Denise Connolly, Fox Chase Cancer Center and Dr. Lorna Rodriguez, Rutgers Cancer Institute of New Jersey.
As a 10 year survivor and someone who has benefited from the research supported by these organizations I am thankful for each and every organization that is making a difference in ovarian cancer research.
Last week, I was invited to speak to the American Medical Student Association (AMSA) chapter at Rutgers University. I drove up to the Busch Campus of Rutgers and parked across the street from the Medical School where the talk was taking place.
I was so pleased to be back on the Banks of the Raritan since both my undergraduate and graduate degrees were from Rutgers.
As the students slowly filtered into the auditorium I spoke to KN, a senior and my contact person for the group, about her plans for a career in medicine. Instead of standing at the podium and speaking as if I was lecturing I decided to sit in a chair at a table in the front of the room. It felt more comfortable sharing my story in that way.
I then began telling my story, interspersing stats and information about symptoms and the importance of having surgery done by a gynecologic oncologist with how I felt when first diagnosed. I shared the hope my gyn oncs provided by simply saying they will do everything to make me well. I thought I would talk about 20 minutes but it ended up being closer to 35 minutes. As I finished my talk I told the future physicians that they should take the time to get to know their patients, and ask them what their goals for the future are. I also told them that they should to be ready to work with others - pharmacists, social workers, nurses to provide the best care for their patients.
When I finished my presentation I asked if anyone had questions. One student asked if I ever got upset or angry with my doctors. I told them the only time I ever got upset was when I had to wait for my CT results. I told them of the time when I was in treatment for my recurrence. I had tried everything to stay calm but eventually ended up calling the social worker and asked her to intervene to get me my results quicker. Waiting for results is difficult but it has become a little easier now that results are posted quickly to health records which can be accessed through a patient portal.
As I gathered up the extra symptom bookmarks and CDC booklets I had brought with me, a few students came up to chat. One young man talked to me about the importance of nutrition for good health. Then a young lady told me she was planning to become a OB/GYN but will now consider becoming a Gynecologic Oncologist after hearing about my relationship with my gyn oncs. That comment made my night. Maybe in 10 years or so I will be reading about this young lady starting her career as new gyn onc in NJ.
Last week Alicia Staley and I presented "Building Community in 140 Characters"at the Eye for Pharma Patient Summit 2015 in Philadelphia. Before we talked about the #bcsm and #gyncsm communities we gave some background on Twitter, hashtags, The Health Hashtag Project and research on twitter communities. Did you know that in June'15:
there were 316 Million monthly Twitter users?
there were 500 Million tweets sent per day?
19% of all adults are on Twitter?
Did you know that the Symplur Healthcare Hashtag Project ( Sept 2015) :
includes almost 8000 healthcare hashtags?
covers over 15,000 healthcare topics?
Did you know that patients have been the driving force behind the cancer hashtags and chats? Examples of patient let communities include: —#BCSM-breast
cancer social media #BTSM-brain
cancer social media #ayacsm-
adolescent & young adult cancer social media #gyncsm-gynecologic
cancer social media —#lcsm-lung
cancer social media #panscm-pancreatic
cancer social media #mmsm-multiple
myeloma social media
We also presented information from the poster Dr Matthew Katz, et al presented at the ASCO 2015 Annual Meeting.
Disease Specific Hashtags for Online Communication about Cancer Care concluded that:
Hashtagscan organize online conversations
about health The
use of organized, cancer-specific hashtags
on Twitter by a
variety of stakeholders in cancer care is not only possible but has
grown Use
of the Cancer
Tag Ontology (CTO) indicates the potential value of online
interaction around specific diseases Further
study is needed to determine
whether the CTO: Improves access
to accurate information or clinically relevant patient outcomes
Alicia Staley presented information about the #BCSM community including this study published in the Journal of Medical Internet Research which found that 67% of the women who initially reported high anxiety
before the chat reported no or low anxiety after participating.
Twitter Social Media is an
Effective Tool for Breast Cancer Patient Education and Support:
Patient-Reported Outcomes by Survey
They concluded that "breast cancer patients' perceived knowledge
increases and their anxiety decreases by participating in a Twitter
Social Media support group.
I presented information about the #gyncsm community including what we learned from our 2014 community survey.
Why
did you
participate?
–To
chat with others with same
interests but from different perspectives
–learn,
share, support
–to
help the community of survivors
—After
participating in the chat:
–41%
of the participants made a change in your personal or
professional routine/practice
–37%
of the participants advocated
for yourself or another
–54%
of the participants used
or refer someone to one of the
resources mentioned in a chat or listed on our blog
In conclusion we noted that:
There
are active, engaged patients who are
helping each other but many also want to be at the table in making changes
in healthcare. Come
find us on Twitter
and listen.
On November 19, 2015 Striving for a Healthier Tomorrow, Today a gynecologic cancer symposium will take place at Mercer County Community College in West Windsor, NJ.
The Symposium is open to health care providers, nurses, survivors, caregivers and community members. This
activity has been submitted for approval to provide 5 CEU Credits.
What:
Medical experts will present discussions on:
Research and newest developments
Cancer prevention and detection
Genetic determinants, risk assessment and management
Gynecologic cancer impact on sexuality and intimacy
Immunotherapy, diagnosis and treatment, improved risk predictors
Patient centered clinical trials
A
panelist of gynecologic cancer survivors will discuss symptom
awareness; personal health choices, fear of recurrence, post-treatment,
and life beyond cancer.
When:
Thursday, November 19th 2015 from 8:00 am - 3:30 pm
The Conference Center At Mercer CollegeMercer County Community College 1200 Old Trenton Rd West Windsor Township, NJ 08550
Last night at Cancer Hope Network's (CHN) Chrysalis Gala, I had the honor of telling my story as an ovarian cancer survivor and a CHN support volunteer . Cancer Hope Network provides one-on-one peer phone support for newly diagnosed or recurrent cancer patients and their caregivers. I have been a support volunteer for over seven years now. Last night at the Hanover Marriott many of CHN's supporters of the past 30+ years were present to celebrate the support provided and to raise funds to continue the support they provide to cancer patients.
Below are the main points I shared with the audience.
2005 started out as a
pretty good year. I was looking forward to
celebrating my 50th birthday at DisneyWorld with family and
friends -12 in all. In late May during my annual visit with my gynecologist I
mentioned a pain I had on the left side of my abdomen. In early June after a
transvaginal ultrasound the pain got worse and I ended up in the ER. After an MRI I learned
my ovaries were enlarged. I was quickly referred to the gynecologic oncologists
at the Rutgers Cancer Institute of NJ.
On July 29th one
month after my birthday my world changed. I woke up from surgery and to learn I
had stage 3B ovarian cancer. I went into that surgery knowing there was a
chance it could ovarian cancer but up to that point I had been more fearful of
being diagnosed with breast cancer. My sister passed away from breast cancer at
the age of 47.
2 weeks after that major
debulking surgery. I started chemotherapy. I chose to be part of a clinical
trial. The trial added selenium to the standard of care - carboplatin and
taxol. It was tough loosing my hair and developing neuropathy but what I was
most upset about was the fact that I had not met one other woman with ovarian
cancer. What made it worse - any time I mentioned ovarian cancer the response
was – Oh Gilda Radner who played Roseanne Roseannadanna on Sat Night live have
ovarian cancer. Yes– she had that disease. But she didn’t live. I also knew the
statistics about women diagnosed with late stage ovarian cancer. Only 30% lived
5 years. I wanted to be in that 30% and I needed to talk to someone who had the
disease and lived.
When I saw a brochure
for Cancer Hope Network in the waiting room of my gynecologic oncologist’s I
picked it up and brought it home. I hesitated at first to call. At the time I
wasn’t too keen on calling anyone and talking about ovarian cancer. But one
afternoon as I laid in bed too tired to get up I went ahead and called.
I told the person who
answered the phone that I just needed to talk to someone who had ovarian cancer
and lived. She took all my information and said she would call back when she
had a match. The very next day she called and said she could connect me right
then and there with a volunteer named Judy. I spent the next half hour talking
to a women diagnosed with stage 3b OC, she lived in NJ, she had the same surgery
and chemotherapy ,her son worked at the college my son was attending, and even
better Judy was a 5 year survivor. It was wonderful. I was not alone. This
meant I could survive too!
When I was out of treatment one year I called Cancer Hope Network and said I
wanted to be one of their support volunteers. I did the training and within a
week or two I was talking to other women with ovarian cancer. I did that until I
recurred on my liver and spleen in 2008 and had to have surgery and more
chemotherapy I had to take a break. But once treatment was done I was back on
the phone able to offer a perspective of being a survivor of recurrent ovarian
cancer. I have been volunteering ever since.
I have spoken to women from NY, Florida, California, Indiana and Kentucky just
to name a few. I have spoken to women treated in the top cancer centers in the
country and those going to small community cancer centers or their local oncologists.
I have talked to women who are a short ride from their doctor’s offices and infusion
centers. And also women who drove eight
hours or took a plane and stayed overnight at hotels when they had treatment. They did all
this to get their life saving treatments.
There were women who
went to in person support groups and others that took part in online groups. But
each and every one of them wanted to talk one –on –one with another survivor
who understood. At some point in most of the conversations I have had after I
have say "I felt that way too"
the reply has always been the same " thank goodness I thought it was just
me."
Thank you Cancer Hope Network for allowing me to provide hope and to give back
to other women the hope and support you gave to me.
I look forward to continuing to volunteer with CHN and to support women diagnosed with ovarian cancer for many years to come.
Dee
Every Day is a Blessing! Blessed to have found CHN when I was initially diagnosed.
In October, I see posts online from women diagnosed with ovarian cancer and other gynecologic cancers complaining and peeved about being surrounded by pink ribbons - on TV , in stores, on shirts, etc. Even women who have breast cancer write about how they see pink ribbons on items that appear to just be a way to sell products. They note that the percentage of money earned from these products actually going to an organization is small.There are other complaints about a large breast cancer non-profit and how so much of the money raised doesn't go to research. Women with metastatic breast cancer are asking to be "seen and heard". They want a greater amount of funds used for metastatic breast cancer research. I can understand why each person complaining or asking for recognition of ovarian cancer feels the way they do. And believe me I have my share of teal shirts , earrings, etc and a few pink things too. In October 2011, I even wrote a post about the "pinking" of the NFL.
My friend Christina and co-moderator of the #gyncsm chat said this on twitter.
fall musings... gyn cancers struggling for basic awareness, breast cancer struggling to move from awareness to action. #gyncsm#bcsm
My life has been impacted by cancer in many ways in addition to my ovarian cancer diagnosis. My sister at the age of 42 was diagnosed with breast cancer and had a mastectomy and chemotherapy. She had a bone marrow transplant when her cancer metastasized. She passed away five years later. It has been twenty years since her passing. And metastatic breast cancer continues to kill women - as does ovarian cancer in the ten years since my diagnosis.
Why is that? Cancer is a very complex disease. After attending medical conferences and listening to researchers I know that. But how does spending money on items that are pink or teal for that matter make a difference?So the next time you make a donation to an organization or buy a product check out how much of the dollars raised actually goes to research.
Let's spend money on research. Because the only way we will be able to understand cancer - breast, ovarian, kidney, lung, pancreatic is through research.
Over the past ten years I have met many women diagnosed with ovarian cancer as well as other gynecologic cancers. Some of these women I interacted with in real life - at events, support groups and through ovarian cancer awareness organizations. Other women I got to know through online groups - Facebook, Inspire or Smart Patients. On this the last day of Gynecologic Cancer Awareness month I write this post to honor those diagnosed as well as to remember the women whose lives were lost to a gynecologic cancer. These women have touched my life.
Christina,co-moderator of #gyncsm chat, and I were discussing all the hashtags used during gynecologic cancer awareness month. Christina had compiled a pretty extensive list which I added 7 hashtags too.
If you have never been to an Ovarian Cancer Survivors Course given by the Foundation for Women's Cancer then you have missed out on a great opportunity to learn the latest about ovarian cancer - what we know about the disease, the lastest and best treatments and how to take care of yourself through all stages of the disease. I have been to three of these courses in the past 10 years, most recently on Sept 16th in Morristown, NJ.
About 75 people attended the course which was held at the Carol G Simon Cancer Center at Morristown Medical Center. There were survivors, caregivers, family, social workers and a number of ovarian cancer organizations in the audience. I was happy to see friends and fellow survivors manning the information tables of the Kaleidoscope of Hope Foundation , the NJ chapter of the NOCC, SHARE and Cancer Support Community.
After a welcome by Dr Daniel Tobias, Director of the Woman's Cancer Center, and listening to his patient, Theresa, discussed how she dealt with her diagnosis, the Course began.
Dr Ilana Cass - Ovarian Cancer:Is Progress Being Made
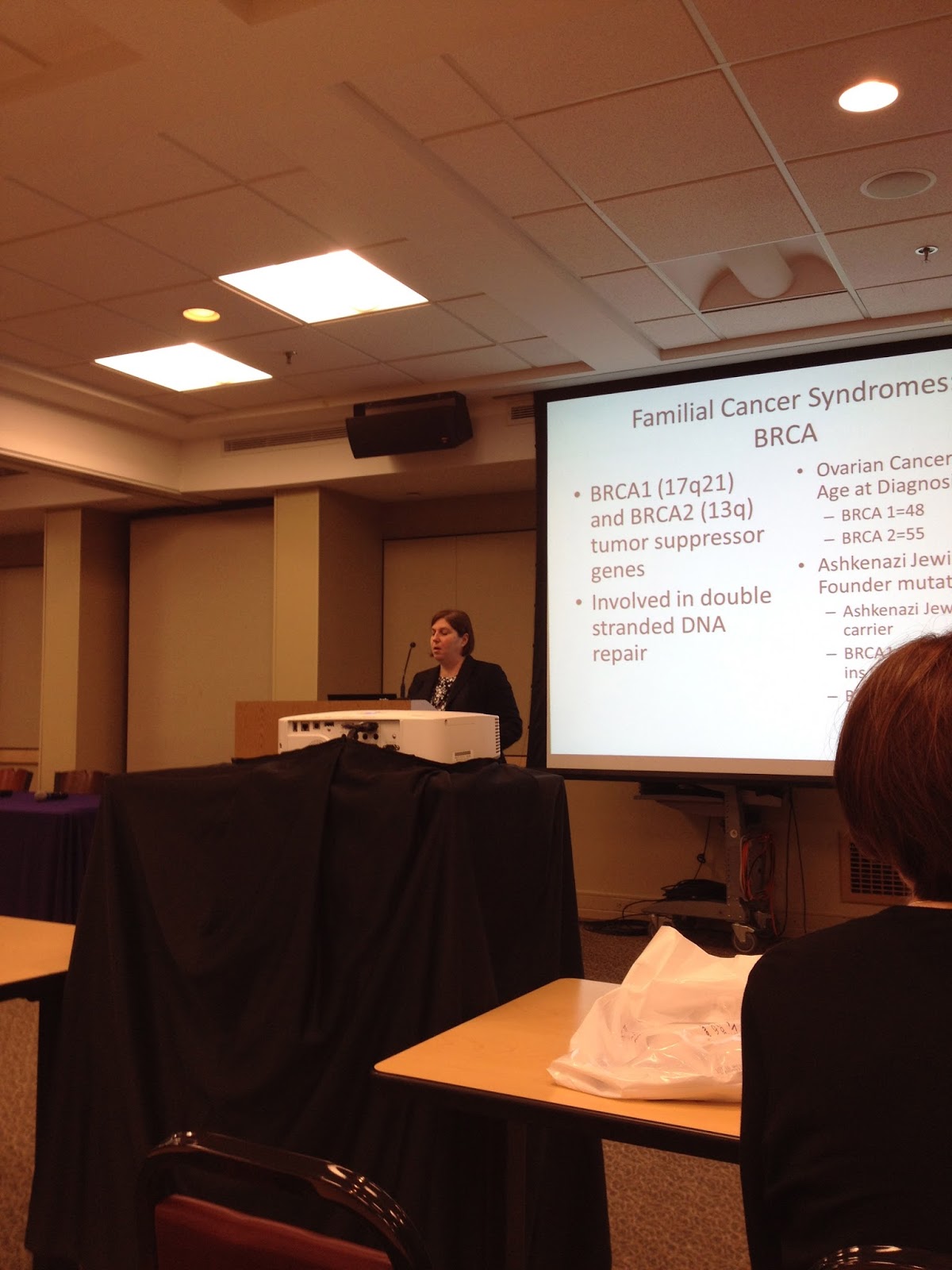
Dr Allison Wagreich -Genetic Risk and Prevention of Ovarian Cancer
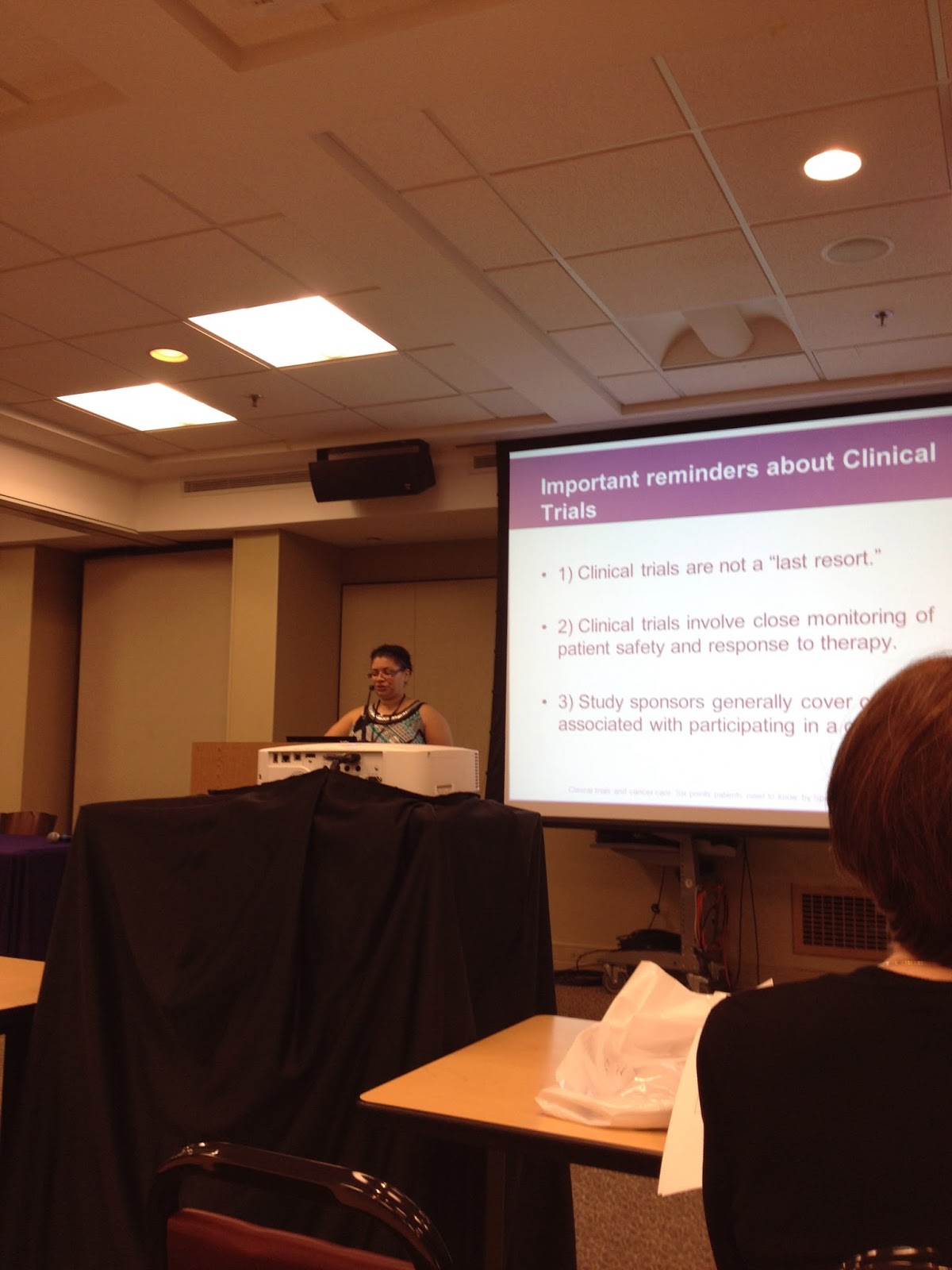
Nana Tchabo -Clinical Trials and New Treatments
Dr Mark Einstein- The Importance of Being Treated by a Gynecologic Oncologists (l) , Dr Micheal Pearl - Supportive Care the Women with Cancer (center) and Dr Daniel Tobias during the question and answer period.
Just a few of the important points shared during the Course :
Surgery by gynecologic oncologists who do large numbers of patients can improve survival.
Neoadjuvant chemotherapy is not inferior to primary debulking surgery.
The Cancer Genome Atlas has provided information on genes responsible for OC.
Exercise can improve quality of life which improves survival.
Familial cancer syndromes include BRCA1,2 and Lynch Syndrome.
3-7% of the women with the BRCA mutations undergoing Risk Reducing Surgery were found to have cancer in their tissue.
Clinical trials are NOT the last resort.
Making progress against cancer is dependent on clinical trials
"Palliative Care is appropriate at any time during management of a serious illness."
Palliative Care is beneficial, improves survival and reduces cost.
Hanging teal ribbons on trees and post signs in towns across this country.
Photo from Turn the Towns Teal website.
I love seeing ribbons as I drive around NJ. Check out their website for more information and put it on your calendar as something to do next year! http://www.turnthetownsteal.org/
In support of Turn The Towns Teal® , Folonari wine and Frederick Wildman and Sons will donate $10,000 to Turn The Towns Teal® for the first 10,000 selfies of people wearing teal on social media that are tagged with #turnmyselfieteal . See http://folonariwines.com/turnmyselfieteal/ for more information.
This campaign in which women ( and some men and even pets) paint their toe nails TEAL was founded by Carey Elizabeth Fitzmaurice (1968- 20015). It is the perfect way to start a conversation about ovarian cancer. I've painted my toes TEAL every September since hearing about it.
Do you know of other unique or fun ways to raise awareness of a gynecologic cancer?
Please let me know and I will add to this page.
For the past few years the CDC has been raising awareness of gynecologic cancers during Gynecologic Cancer Awareness month. They have done this through print ads and public service announcements on the radio and TV. This year's PSA is Cote de Pablo speaking about cervical cancer and getting tested.
There are symptoms for gynecologic cancers which the CDC highlights in this year's PSA "Are you Listening" .
In 50 States of Teal: Ovarian Cancer Care Across America OCNA has evaluated the performance of each state in the US in 10 areas of ovarian cancer care. The metrics include prevention, treatment, survivorship, and end-of-life care.
New Jersey scored 8 out of 10 and better than 42 other states.
When I was diagnosed with ovarian cancer I decided to learn as much as I could about the disease. While I was in treatment I was offered genetic testing for BRCA1 and 2 which I accepted. Our knowledge about the genetics of ovarian cancer has grown tremendously over the past ten years. Let's start with this basic video from the NCI on genetics and cancer.
Now let's talk about ovarian cancer in particular.
About
15% of the ovarian cancers diagnosed are due to germline (inherited and passed
on to offspring) mutations in the BRCA1
and BRCA2 genes. Having these mutations increases the risk of ovarian cancer by
15-50%. “Nearly one-third of women with
hereditary ovarian carcinoma have no close relatives with cancer, and 35% of
women with hereditary ovarian carcinoma are older than 60 years at diagnosis”( NCI) . The remaining
ovarian cancers are due to what we call sporadic or somatic mutations.
Following the BRCA mutations the next inherited syndrome that leads to ovarian cancer is Lynch Syndrome. Mutations in the MLH1, MSH2, MSH6, PMS2 and
EPCAM genes are linked to Lynch Syndrome. Women who have Lynch syndrome have an estimated 9-12 %
lifetime risk for developing ovarian cancer. (http://www.cancer.net/cancer-types/lynch-syndrome)
In
June 2011, the The Cancer Genome Atlas (TCGA) Research
Network issued the results of whole-exome sequencing of ovarian cancer tumors. They examinesd the
protein-coding regions of the genome, of 316 ovarian cancer tumors.
21
percent of the tumors studied showed mutations in BRCA1 and BRCA2
six
other statistically recurrently mutated genes: RB1, NF1, FAT3,
CSMD3, GABRA6 and CDK12. CDK12 is involved in RNA
splicing regulation
96%
of ovarian cancers had a T53 mutation. T53 controls a tumor suppressor protein
that stops cancer from forming
108
genes were associated with poor survival
85
genes were associated with better survival
68
genes that could be targeted by existing Food and Drug Administration-approved
or experimental therapeutic compounds
Four
related subtypes of ovarian cancer based on the patterns of DNA methylation—a chemical reaction
in which a small molecule called a methyl group is added to DNA, changing the
activity of individual genes.
The
SGO released a Clinical Practice statement in 2014 stating that all women
diagnosed with ovarian, tubal and primary peritoneal cancer regardless of age
or family history should receive
counseling and offered a genetic test. (https://www.sgo.org/clinical-practice/guidelines/genetic-testing-for-ovarian-cancer/
) Knowing a women has a BRCA mutation may
allow her to receive PARP inhibitor treatment . Olaparib was recently approved
by the FDA to treat women with recurrent ovarian cancer.
The more researchers understand the genetics of ovarian cancer the better they can develop drugs to treat specific mutations and the more personalized women's treatment can become.