Teal is the awareness color of ovarian cancer. Women of Teal is a play on the words "Man of Steel" used to describe Superman. I have found my fellow ovarian cancer survivors to be the strongest, most helpful women in the world. They are truly Women of Teal!
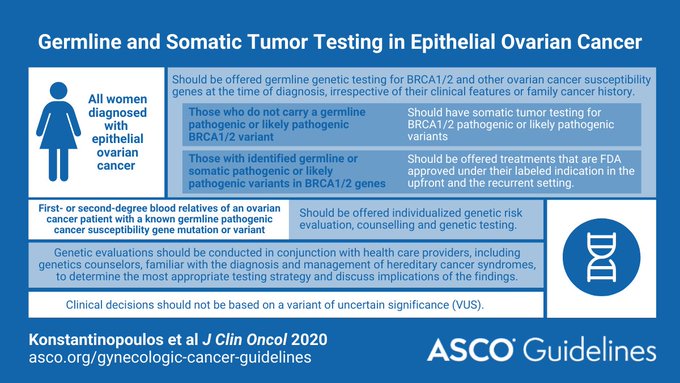
"All women diagnosed with epithelial ovarian cancer should have germline genetic testing for BRCA1/2 and other ovarian cancer susceptibility genes
In women who do not carry a germline pathogenic or likely pathogenic BRCA1/2 variant, somatic tumor testing for BRCA1/2 pathogenic
or likely pathogenic variants should be performed.
Women with
identified germline or somatic pathogenic or likely pathogenic variants
in BRCA1/2 genes should be offered treatments that are US Food
and Drug Administration (FDA) approved in the upfront and the recurrent
setting.
Women diagnosed with clear cell, endometrioid, or mucinous
ovarian cancer should be offered somatic tumor testing for mismatch
repair deficiency (dMMR).
Women with identified dMMR should be offered
FDA-approved treatment based on these results.
Genetic evaluations
should be conducted in conjunction with health care providers familiar
with the diagnosis and management of hereditary cancer. First- or
second-degree blood relatives of a patient with ovarian cancer with a
known germline pathogenic cancer susceptibility gene variant should be
offered individualized genetic risk evaluation, counseling, and genetic
testing.
Clinical decision making should not be made based on a variant
of uncertain significance.
Women with epithelial ovarian cancer should
have testing at the time of diagnosis. "
February 28th is Rare Disease Day® .Rare Disease Day is an
annual awareness day dedicated to elevating public understanding of rare
diseases and calling attention to the special challenges faced by patients and
the community.
In
the United States, a disease is considered rare if it is believed to affect
fewer than 200,000 Americans.Nearly 1 in 10 Americans live with a rare
disease—affecting 30 million people—and two-thirds of these patients are
children.
Do you know which diseases are considered rare diseases by the NIH's Office
of Rare Diseases Research? The following ovarian cancers are considered rare:
To learn more about any of those ovarian cancers just click on the name above.
Rare Disease Day takes place every year
on the last day of February (February 28 or February 29 in a leap year)—the
rarest date on the calendar—to underscore the nature of rare diseases and what
patients face. It was established in
Europe in 2008 by EURORDIS, the organization representing rare disease patients
in Europe. Rare Disease Day is sponsored in the U.S. by the NationalOrganization for Rare Disorders (NORD)®, a leading independent, non-profit
organization committed to the identification, treatment, and cure of rare
diseases.
If you are on social media and have a rare disease you can use this template and show your stripes on this Thursday , February 28th. My stripes are rare. I have _____, a #raredisease. #ShowYourStripes #RareDiseaseDay {upload photo of yourself}
I'll be sharing this blog post as a way to raise awareness. Dee Every Day is a Blessing!
Earlier this month the FDA approved the expanded use of Avastin (bevacizumab) for platinum sensitive ovarian cancer (OC) . Being platinum sensitive means that a women has a recurrence 6 months or more from her last treatment.
Avastin may be used for:
"Recurrent epithelial ovarian , fallopian tube or primary peritoneal cancer that is
platinum-resistant in combination with paclitaxel, pegylated liposomal doxorubicin, or topotecan
platinum-sensitive in combination with carboplatin and paclitaxel or in combination with carboplatin and gemcitabine, followed byAvastin as a single agent (1.6) "
The complete label of use for Avastin / bevacizumab may be found here.
This approval is based on two phase III studies. One study, GOG-213, showed a 5 month longer overall survival for women with platinum sensitive OC when treated with bevacizumab and chemotherapy versus chemotherapy alone. The other study, OCEANS, showed a median progression free survival of 4 months for those receiving Avastin and chemotherapy versus those receiving placebo and chemotherapy.
Avastin had previously been approved in 2014 for women with platinum resistant ovarian cancer, fallopian tube and primary peritoneal in combination with paclitaxel, pegylated liposomal doxorubicin or topotecan chemotherapy.
Dee
Every Day is a Blessing! Happy to see more options for women with platinum sensitive OC.
Last June, when I attended the ASCO annual meeting I was fascinated by a presentation by Dr Usha Menon on the UK Collaborative Trial of Ovarian Cancer Study (UKCTOCS) using the ROCA (Risk of Ovarian Cancer Algorithm) test. I wrote about it here.
Earlier this month I was contacted by a representative of the PR firm that is representing Abcodia, a company that develops early detection tests for cancer. On December 2, 2015 Abcodia launched the ROCA (Risk of Ovarian Cancer Algorithm) test here in the US. After finding and reading my blog, the firm contacted me to share that the test was now available. Of course I was interested in learning more about this test that was now available in 5 states - Texas, Massachusetts, Illinois, Arizona and my home state of New Jersey. You can find the press release at http://www.abcodia.com/news_021215.php.
We conversed via e-mail and then I had a teleconference with the PR firm's representative as well as the representatives from Abcodia. Abcodia's responses to my questions are shown below in quotes and italics. I have permission from Abcodia to share the information provided.
What is the difference between the ROCA test and the CA-125, which is one component of the ROCA test? "The ROCA Test does not use CA-125 with a fixed cutoff, instead, ROCA establishes a patient’s baseline, and then evaluates her CA-125 pattern over time." (CA-125 uses a fixed cut-off of either 35 u/ml or 20 u/ml depending on which test protocol is followed. "ROCA incorporates the CA-125 result (and all the following CA-125), and, factors in age, menopausal status and high risk factors, which affect CA-125 levels. ROCA takes all of this data on one patient and creates a unique profile for her. ROCA then compares her profile to known profiles in a database of thousands of women to see if her profile more closely resembles that of women who have cancer or women who do not have cancer. The ROCA Test reports a numerical score which represents a woman’s risk of having ovarian cancer (e.g. 1 in 5,000) now. The risk score is categorized as Normal, Intermediate or Elevated as a guide for clinical decisions by your doctor."
Who is the ROCA test meant for and when should they have it? The ROCA test is meant for women in the general population who are "Between 50 and 85 years and have been through menopause; or" high risk women "Between 35 and 85 years with a family history of ovarian and/or breast cancer, are of Ashkenazi Jewish descent with a known family history of ovarian or breast cancer, or have tested positively for BRCA1, BRCA2 or Lynch syndrome gene mutations." The CA-125 may be used for high risk women only. The test would be similar to "Routine testing, just like you would a physical or mammogram." Currently the CA-125 with a fixed cutoff is sometimes used for high risk women only when advised by their physicians. As many of my readers know, the CA-125 is used by gynecologic oncologists to manage the care of women who have been diagnosed with ovarian cancer.
How does the ROCA test compare to the CA-125 in terms of how well it detects ovarian cancer?"When combined with appropriate clinical follow-up, the ROCA Test has been shown to detect more than twice as many ovarian cancers before the current CA-125 35U/ml fixed cutoff. As a screening tool by itself, CA-125 is not reliable and has not been shown to improve outcomes for women with ovarian cancer."
How does a woman go about getting the test? She fills out a form online to see if she is eligible and orders the kit. Then she finds a referring physician (OB-GYN or primary care physician) to sign the request for the test and the blood work. "Abcodia is proactively educating OBGYNs, has a dedicated phone line and online materials specifically for healthcare professionals."
What is the cost of the test and is it covered by Medicare, other insurances? "The cost of each ROCA Test is $295. This includes the cost for the Iggbo blood draw service, who will have a trained phlebotomist come to a doctor’s office, a patient’s home or other location of the patient’s choice to draw blood. Iggbo will then ship the blood sample via FedEx to Abcodia’s laboratory." Abcodia's lab is a CLIA, registered lab. Currently the test is not covered by Medicare or other insurances. "Abcodia does plan to seek regulatory and reimbursement approvals"
Can a woman get the CA-125 drawn at a different lab and then submit it to Abcodia? It is recommeded that the blood draw be through Abcodia's blood draw partner, Iggbo. A patient can have her blood drawn at her physician's office or a hospital if a phlebotomist is available. All samples do need to be tested at the Abcodia lab to insure there is no lab to lab variability. CA-125 test results from other labs (Quest, Labcorp) for use with the test are not accepted.
What happens after the initial result? "The frequency of the ROCA test will be determined by the woman's doctor based on her risk factors for ovarian cancer and the ROCA test result. Post menopausal women with no additional risk factors will likely have one test per year. Women at high risk for ovarian cancer , will complete the test more frequently, at a minimum three times per year and may include a Transvaginal Ultrasound (TVU). If the result falls outside of the normal range(intermediate or elevated) a doctor may recommend a repeat ROCA test within the next six weeks to three months.Patients may also be referred for a transvaginal ultrasound scan of the ovaries or other possible clinical assessments. "
Does the women pay $295 each time she has a follow-up test?"After a patient takes her first test, Abcodia offers the patient several options: 1. The patient can pay per test ($295) for each test. 2. The ROCA Test Subscription: one for high risk patients and one for the general population. Abcodia will offer patients a 2 year subscription that includes the Iggbo blood draw, repeat ROCA tests and TVU (Transvagina Ultrasound) as a result of intermediate, elevated or severe ROCA result. 3. Interest free payment plans."
Why is the test available in only five states ?Starting in five states will allow the test process to be optimized. The delay with other states is due to each individual state's permit application period and process. Some are longer than others.
This video is an overview of how the ROCA test works.
I have charted my CA-125 results since my initial diagnosis. So monitoring the trends in CA-125 makes sense to me. But there is one caveat, there is a small percentage of women, like myself, who have a CA-125 result that is normal and disease may be still present. My CA-125 was normal at 17 u/ml, when I learned via CT scan that I had recurred on my liver and spleen. So woman whose CA-125 does not rise may not benefit from this type of screening.
I still had a few questions about applying this test to the general public. I wondered if the ROCA test would find the disease at an earlier stage and if the survival would be longer for women whose disease was detected by this test. I did not have to wait too long for some of the answers because on December 17th the results were published in the Lancet journal.
When I first heard I had ovarian cancer I didn't know that there were multiple types. I didn't realize that some cancers were on the surface of the ovary , some were in the egg cells and some were on the follicles. I learned that each of the main types of ovarian cancer had sub-types. Below is a list of the different types of ovarian cancer.
Epithelial Ovarian
Cancer ( Forms in the tissue covering the ovary)
Subtypes:
Serous
mucinous
clear cell
endometrioid
transitional cell
Germ Cell Ovarian
Cancer ( forms in the egg cells of the ovary)
Teratoma
Mature cystic
terotoma
Immature teratoma
Mondermal teratoma
dysgerminoma
yolk sac tumor
embryomal carcinoma
choriocarcinoma
Sex Cord
Stromal(forms in the sex cord/ ovarian follicles)
It is important that
if you are diagnosed with ovarian cancer you know the exact type. The exact type of
cancer you have will help determine the best treatment for you.
A study looking at characteristics of women who are long-term survivors of ovarian cancer was recently published in the journal Obstetrics & Gynecology . The study " Characteristics of Long-Term Survivors of Epithelial Ovarian Cancer" is currently pre-published online and I am happy to say you can read the entire article for free. So I took the opportunity to download the article and read it and looked at the data.
This study is a retrospective study of over 11,500 women in California diagnosed between 1994 and 2001 with epithelial ovarian cancer. The California Cancer Registry was used. Thirty one percent of the women in the study were long term survivors. Since I reached 10 years of survivorship last month I was interested to see how my characteristics matched those of women in California who were long term survivors.
The study found the predictors of long-term survival were younger age ( 18-50) early stage low grade non-serous Out of all those predictors I have one characteristic - younger age - and I barely made that one. I was diagnosed one month after my 50th.
I found it interesting that 1/3 of the long term survivors were women who were late stage /high grade serous. The authors explained this result as better surgical techniques that offered these women advantages as well as possible IP or BRCA mutation status. But that information was not available in the data set studied. I appreciate that the authors made note of the issues associated with long term survival. The paper ends with this paragraph- " Long-term survival may bring its own challenges beyond worry about recurrence. Studies have shown that patients with ovarian cancer are challenged with problems of anxiety, fatigue, sexual, social, and financial problems, which should be amenable to appropriate interventions. These studies highlight that physicians, especially those who provide primary care, should be prepared to address cancer survivor- ship needs in this group of patients. " It would be interesting to see if similar studies were conducted in other states if the characteristics would be the same. Dee Every Day is a Blessing!
This post will also be appearing on the SGO blog page.
I don’t know who coined the term cancerversary
but I have been using it for a few years. For some survivors their cancerversary is the anniversary of the
day they were diagnosed with cancer. Yet for others it is the anniversary of
the day they finished treatment.
I celebrate my cancerversary on the day I was diagnosed. I remember that day quite
vividly. I also remember the words my gynecologic oncologist, said to me in the
hospital recovery room. It was around noon on Friday, July 29, 2005. She said,
"Dee, I am sorry. I found ovarian cancer. You are stage 3B.” Then
she went on to say, “But I will do my best to make you well." And that is
what she and her colleagues at the Rutgers Cancer Institute of NJ have done. They made me well in
2005 and again in 2008 when I recurred on my liver and spleen. They continue to
make me well to this day helping me through the side effects of chemotherapy
and dealing with the fear of recurrence. They are my lifesavers.
As I celebrate my eighth cancerversary on July 29th I want to thank my
gynecologic oncologists, Dr. Gibbon and Dr. Rodriguez and all gynecologic
oncologists who provided such outstanding and compassionate care to me and countless of women
diagnosed with gynecologic cancers.
A few days ago the results of a very large study was published. The study by the Collaborative Oncological Gene-Environment Study (COGS) involved over 200,000 participants and hundreds of researchers from around the world. Here is a link to the overview article in Nature. It looked at the genetic markers for breast, prostate and ovarian cancer. The study was reported in 13 articles in 5 journals but I concentrated on finding just the ovarian report. I searched online and found the article "GWAS meta-analysis and replication identifies three new susceptibility loci for ovarian cancer" in Nature Genetics. I looked through the researcher names and out popped Dr Lorna Rodriguez-Rodriguez. I was thrilled to read that one of my gynecologic oncologists at the Cancer Institute of New Jersey was involved in the research. I allowed my tumor to be studied for the clinical trial I participated in so I wonder if my tumor was part of this large genetic analysis. I'll have to ask Dr R the next time I see her. In a nutshell the Genome Wide Association Study (GWAS) found 4 locations in the DNA that were susceptible for epithelial ovarian cancer. All of the locations were associated with the serous type of epithelial Ovarian Cancer ( EOC) . In the discussion of the results the researchers report:
"Molecular analyses of genes at these loci ( Location of a gene), combining publicly available data sets and systematic, large-scale experiments, point to a small number of candidate gene targets that may have a role in EOC initiation and development. However, the effects of the new susceptibility loci were modest, and together they explain less than 1% of the excess familial risk of EOC, with about 4% being explained by all known loci with common susceptibility alleles." (An allele is one of two versions of a gene.)
"Fewer common susceptibility loci have now been found for EOC than for several other common cancers, including breast, colorectal and prostate cancers28. It seems unlikely that the underlying genetic architecture for EOC susceptibility is substantially different from those of other cancers. This suggests that a key factor limiting our ability to detect susceptibility loci is sample size—the power of this study to detect risk alleles across a range of effect sizes was modest (Supplementary Fig. 12). However, EOC is less common than these other cancers and has a higher mortality rate, and recruiting extremely high numbers of cases will be difficult." The more tumor samples researchers can examine the more we can learn about how epithelial ovarian cancer develops. Now is the time for more women with all types of ovarian cancer to allow their tumor cells be used for studies like this one. I've given my tumor tissue to research . Will you? Dee Every Day is a Blessing
Continued research by Dr. Joanne Weidhaas has resulted in a recent journal article that further establishes the KRAS gene mutation as a predictor of poor outcomes and chemotherapy resistance for women with epithelial ovarian cancer. Let's step back a bit. The KRAS gene is the "v-KI-ras2 Kirsten rate sarcoma viral oncogene homolog". So glad they use the KRAS abbreviation. It is also know as an oncogene because a change in its makeup can cause a cell to become cancerous. The KRAS gene produces the KRAS protein which controls cell division. It is a part of the signaling pathway RAS/MAPK . The protein signals whether or not the nucleus should divide or not.The KRAS protein acts like an on off switch . It is turned on when it binds with the molecule GTP. When it converts GTP to GDP it is turned to an off position . In the article "A KRAS variant is a biomarker of poor outcome, platinum chemotherapy resistance and a potential target for therapy in ovarian cancer" The authors found that post menopausal women with the Epithelial Ovarian Cancer and this gene mutation were more likely to be platinum resistant and to die from the disease. This information certainly opens the door to developing new treatment options for women with the mutation. Dee Every Day is a Blessing! Sources :Genetics Home Reference a service of the US National Library of Medicine
What is ovarian cancer ? Ovarian Cancer forms in the tissue of the ovaries the female reproductive glands. We are still not sure how or why ovarian cancer forms. (Note:Recent research proposed that ovarian cancer forms in the fallopian tubes. ) But not every ovarian cancer is the same as every other ovarian cancer. The most common form is Epithelial, then Germ cell and then Sex Cord Stromal. Each of these has subtypes.
Epithelial Ovarian Cancer ( Forms in the tissue covering the ovary)
serous
mucinous
clear cell
undifferentiated
mixed epithelial
endometrioid
Germ Cell Ovarian Cancer ( forms in the egg cells of the ovary)
teratoma
dysgerminoma
yolk sac tumor
embryomal
choriocarcinoma
Sex Cord Stromal(forms in the sex cord/ ovarian follicles)
granulosa cell
Sertoli-Leydig
Source:John Hopkins Pathology (http://ovariancancer.jhmi.edu/home.cfm). The site offers excellent description of each of these different types and subtypes.
It is important that if you are diagnosed with ovarian cancer you know the type . The type of cancer you have may influence the treatment you have.
After writing the last post about CA-125 I started to think about what causes the differences between ovarian cancer tumor cells. Why is cancer antigen CA-125 ,a protein , not elevated (or not being produced at the same level by my cancer tumor cells) as compared to other women who have been diagnosed at the same stage.
When I attended the ASCO meeting, I learned that there are many different subtypes of ovarian cancer. Many more than those I was initially aware of. So I put together a list of the different types of ovarian cancer.
What type/ histology is your ovarian cancer tumor?
So it seems that even if you have the most common type of ovarian cancer, epithelial, your cells may be different than a friends since you may have a different sub-type. The ovarian cancer cell type along with the stage is important in determining the type of treatment you will be offered, so knowing that information is important.
I know what subtype I am. What subtype are you? Check your pathology report or ask your doctor. It is good knowledge to have.